Lung Cancer Staging According to TNM9th Edition
Lung Cancer Staging According to TNM 9th Edition (IASLC, 2025)
Introduction
The TNM system provides a standardized way to describe the anatomical extent of cancer. Using a common nomenclature improves communication about prognosis, treatment decisions, and comparability of outcomes across patients and studies. The lung cancer TNM system covers both non–small cell lung carcinoma (NSCLC) and neuroendocrine tumours of the lung (ranging from typical carcinoid to small cell lung carcinoma). It is not intended for pulmonary sarcomas, lymphomas, or other rare thoracic neoplasms.
Epidemiology of Lung Cancer
Lung cancer is a malignant disease that originates in the tissues of the lung, most often in the cells lining the airways. Over time, genetic and cellular changes lead these cells to grow uncontrollably, invade surrounding tissues, and ultimately spread (metastasize) to other organs. Historically, lung cancer was a rare diagnosis prior to the widespread use of tobacco in the 20th century. With the rise of cigarette smoking and industrial exposure, the incidence of lung cancer surged dramatically.
Today, lung cancer ranks among the most common cancers worldwide and is the leading cause of cancer-related death in both men and women. In 2020, an estimated 2.2 million new cases and approximately 1.8 million deaths occurred globally, representing about 11–12% of all new cancers and nearly 18% of cancer deaths. In the United States alone, rates show that lung and bronchus cancers account for around 11% of all new cancer diagnoses and are responsible for over 20% of all cancer deaths. Typically, the average age at diagnosis is around 70 years old.
Major risk factors include tobacco smoking (responsible for ~80–90% of lung cancer cases), secondhand smoke, radon exposure, occupational carcinogens (such as asbestos), and air pollution. Because lung cancer often presents at advanced stages when symptoms arise, its prognosis remains poor despite advances in imaging, surgical, systemic and targeted therapies.
Key Changes in the 9th Edition
Compared with the 8th edition the revisions are modest. The main differences are:
- T component: no changes.
- N component: N2 is subdivided into N2a (single ipsilateral mediastinal/subcarinal station) and N2b (multiple ipsilateral mediastinal/subcarinal stations).
- M component: M1c is split into M1c1 (multiple metastases confined to a single organ system) and M1c2(metastases involving more than one organ system).
These updates lead to adjustments in several stage groupings (notably within IIA, IIB, IIIA and IIIB).
Prefixes and Evaluation Codes
TNM categories are often prefixed to indicate context:
- c — clinical stage (pre-treatment, all available clinical/imaging data).
- p — pathologic stage (based on surgical resection specimen only).
- y — post-treatment (used for restaging after systemic therapy or radiotherapy; ycTNM if no resection, ypTNM if after resection).
Additionally, an E code may describe the type of information used for staging:
- E1: physical exam
- E2: imaging
- E3a: cytology; E3b: histology
- E4: resection specimen
Examples:
- cT2aN2aM0 E3a — clinical staging using cytologic confirmation of nodal disease.
- pT1cN0M0 E4 — pathologic staging after resection.

Subsolid Lesions (Ground-Glass / Part-Solid)
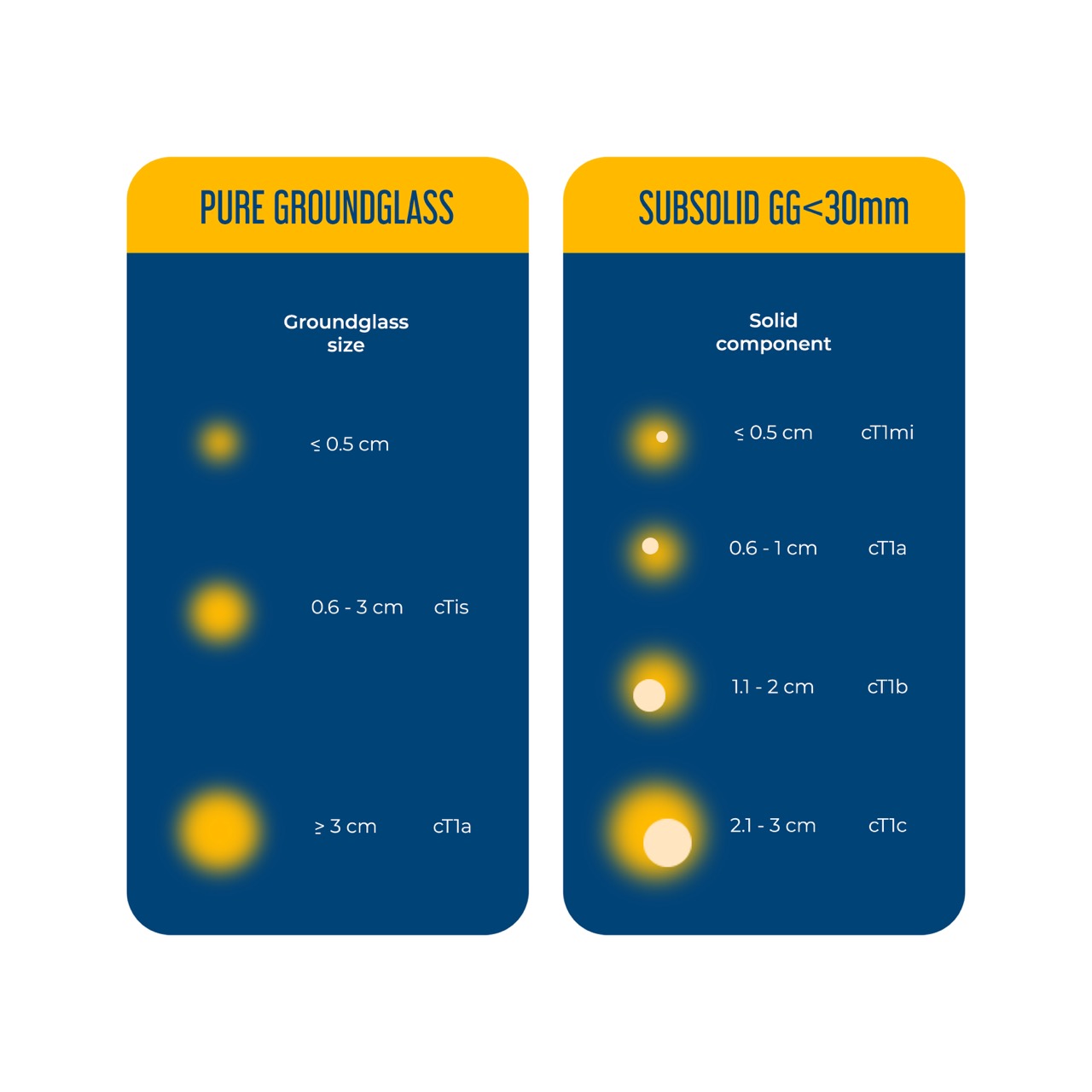
Subsolid lesions show ground-glass attenuation on CT and typically reflect a lepidic growth pattern. They may be purely ground-glass or part-solid (containing a solid component that usually corresponds to invasion on histology).
Reporting essentials: both the total lesion diameter and the maximum diameter of any solid component must be recorded on contiguous thin-section (≤1.5 mm) CT images in the lung window.
Pure ground-glass lesions
- If total diameter ≤ 30 mm → classify by total size and at most cTis (in situ).
- If total diameter > 30 mm → lesion is at least cT1a, regardless of being pure ground-glass.
Part-solid lesions (solid component present)
- Staging is based on the greatest dimension of the solid component (as a surrogate for the invasive part).
- Example: total ≤30 mm with solid ≤5 mm → cT1mi (minimally invasive). If total >30 mm with the same ≤5 mm solid, the lesion is cT1a (because total >30 mm triggers cT1a).
- Solid component 11–20 mm → cT1b; 21–30 mm → cT1c.
T-Staging (Tumor size and local invasion)
T category uses the largest diameter of invasive tumor (pathology or radiologic solid component). Measurements can come from multiplanar reconstructions if larger than axial measurements.
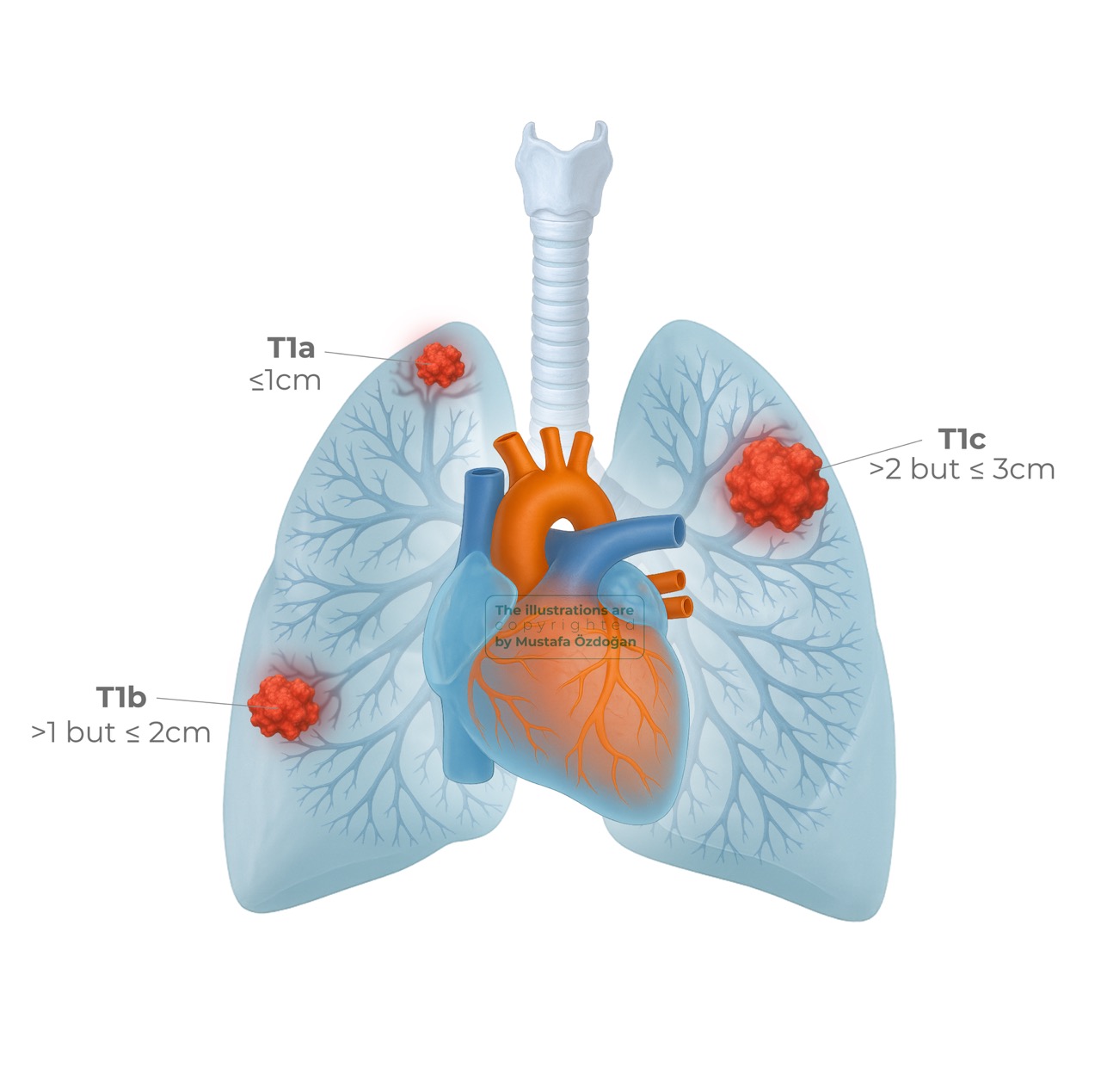
T1: ≤ 3 cm, located within lung parenchyma or in a lobar/peripheral bronchus.
- T1mi — minimally invasive adenocarcinoma
- T1a — ≤ 1 cm
- T1b — > 1 cm and ≤ 2 cm
- T1c — > 2 cm and ≤ 3 cm
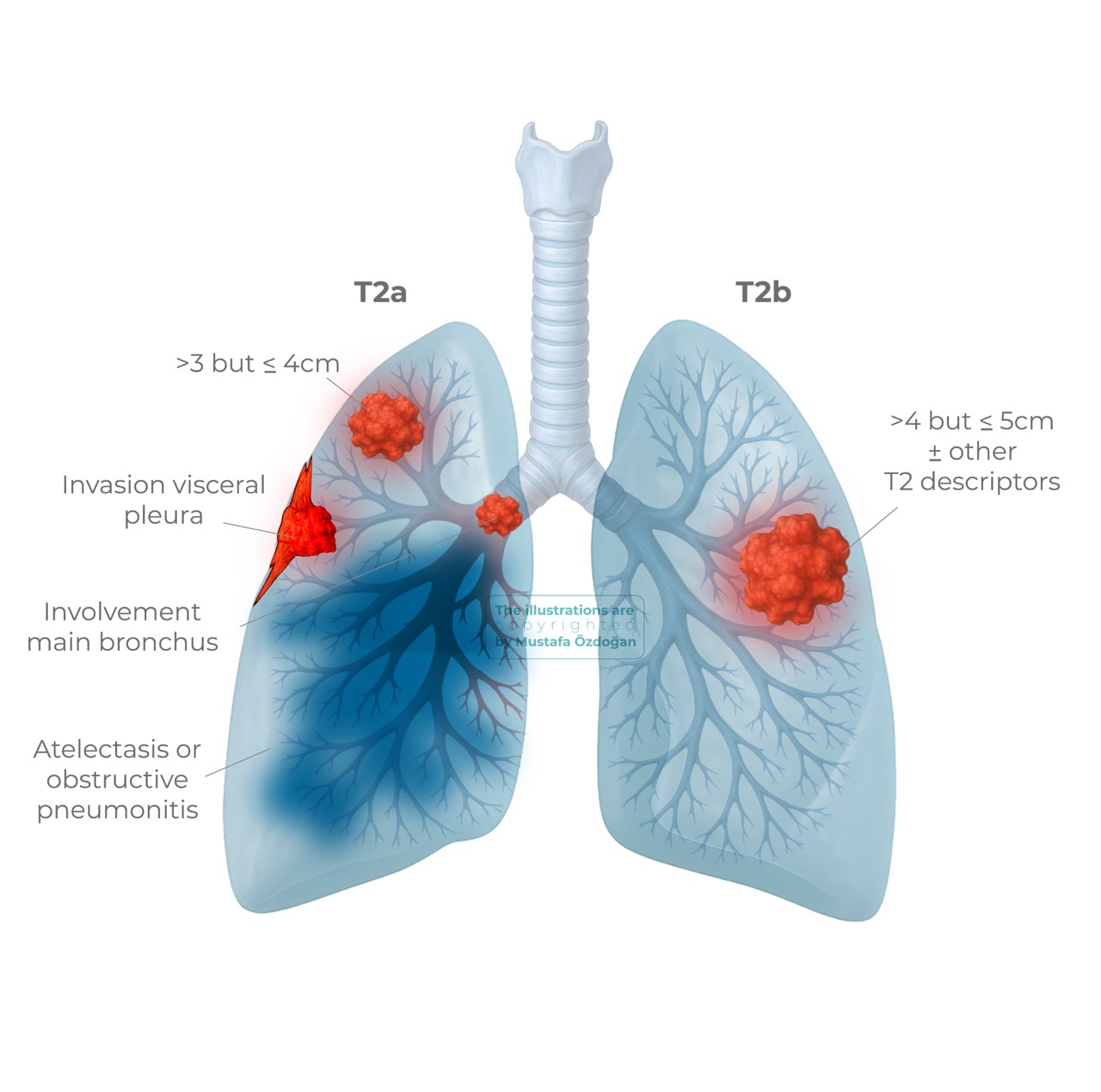
T2: > 3 cm and ≤ 5 cm or tumors with specified features:
- T2a — > 3 cm and ≤ 4 cm; or tumor that invades visceral pleura, involves main bronchus (distal to carina), or causes atelectasis/obstructive pneumonitis extending to the hilum.
- T2b — > 4 cm and ≤ 5 cm (with or without other T2a features).
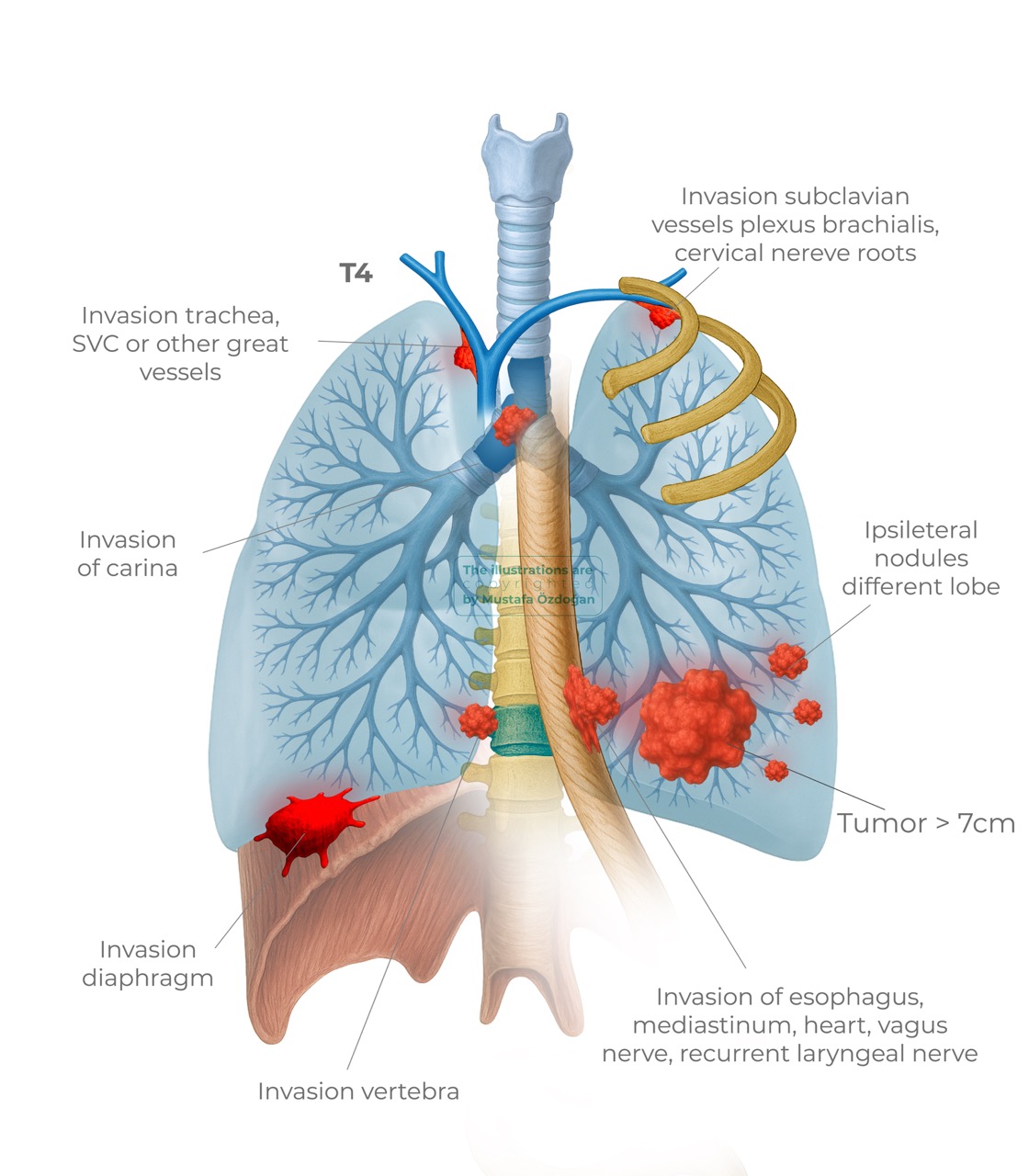
T3: > 5 cm and ≤ 7 cm; or invasion of parietal pleura or chest wall; or invasion of pericardium, phrenic nerve, azygos vein, thoracic nerve roots/stellate ganglion; or separate tumour nodule(s) in the same lobe.

T4: > 7 cm; or invasion of mediastinum, trachea, carina, esophagus, diaphragm, heart, great vessels, intrapericardial pulmonary vessels, vertebral body, spinal canal, cervical nerve roots, brachial plexus; or separate tumour nodule(s) in different ipsilateral lobe(s).
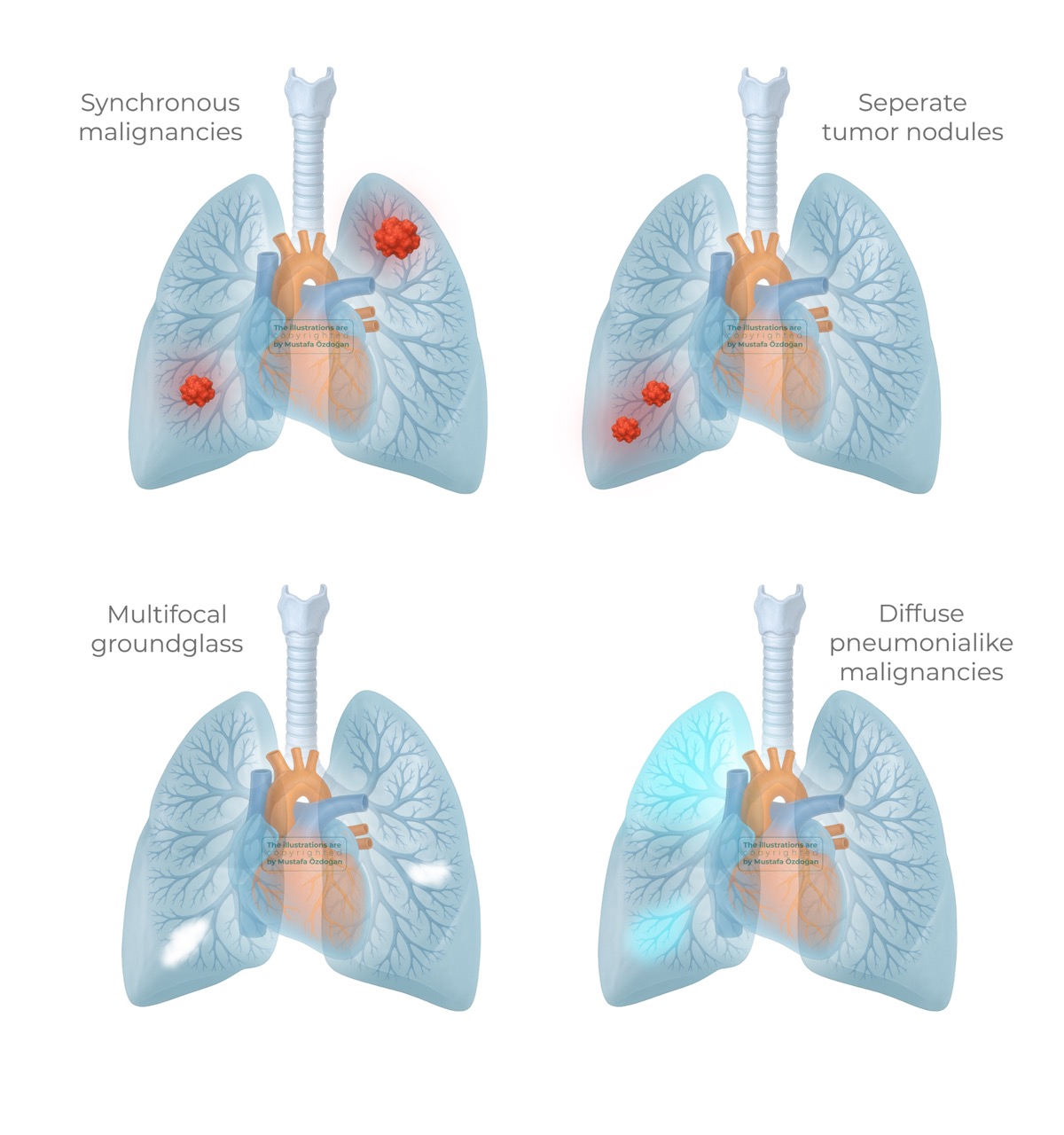
Staging Multiple Pulmonary Lesions
1. Synchronous primary tumours: assign a separate TNM stage to each tumour (treat independently).
2. Separate nodules of the same tumour:
- same lobe → T3
- same hemithorax, different ipsilateral lobe → T4
- contralateral lobe → M1a
- single N and single M are assigned for the patient.
3. Multiple ground-glass / lepidic lesions: stage according to the dominant (most T-dominant) lesion; single N and M. Multiplicity is documented as number.
4. Diffuse pneumonia-type adenocarcinoma: apply the same nodal and metastatic rules (same lobe → T3; same side, different lobe → T4; contralateral lobe → M1a); single N and M assigned.
N-Staging (Regional Lymph Nodes)
Regional nodal stations include intrathoracic nodes and supraclavicular/scalene nodes per the IASLC map. Uncommon nodes (parasternal, axillary) are considered non-regional (metastatic).
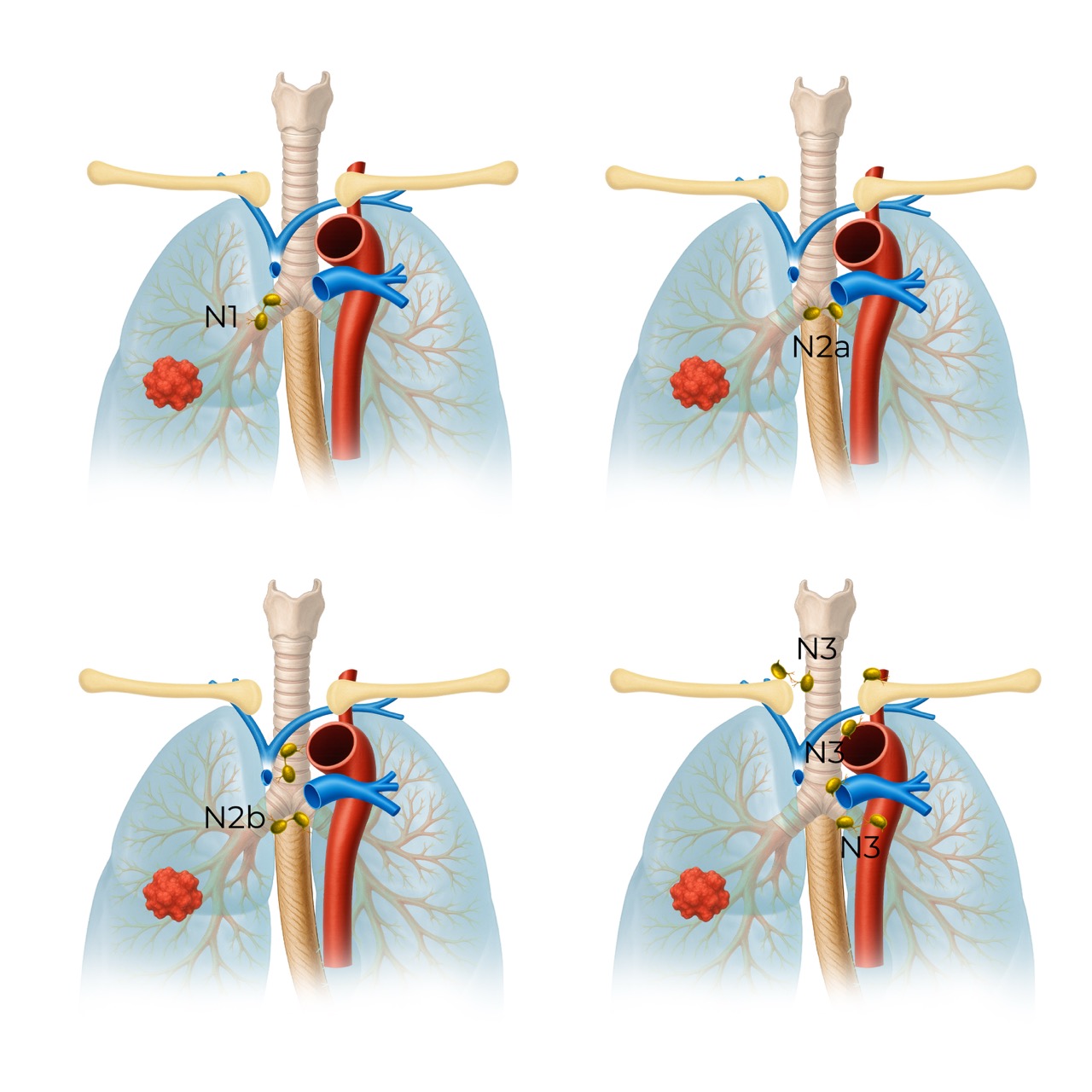
N1 - N3 nodes
- N1 Metastasis in ipsilateral intrapulmonary, peribronchial or hilar lymph nodes, including nodal involvement by direct extension.
- N2a Metastasis to a single ipsilateral mediastinal or subcarinal lymph node station.
- N2b Metastasis to multiple ipsilateral mediastinal and/or subcarinal lymph node stations.
- N3 Metastasis in contralateral hilar or mediastinal lymph nodes or in scalene or supraclavicular lymph nodes.
Regional Lymph Node Classification System
Regional lymph node involvement in lung cancer includes the intrathoracic, scalene, and supraclavicular nodes. Less common involvement of for example parasternal or axillary nodes is regarded metastatic.
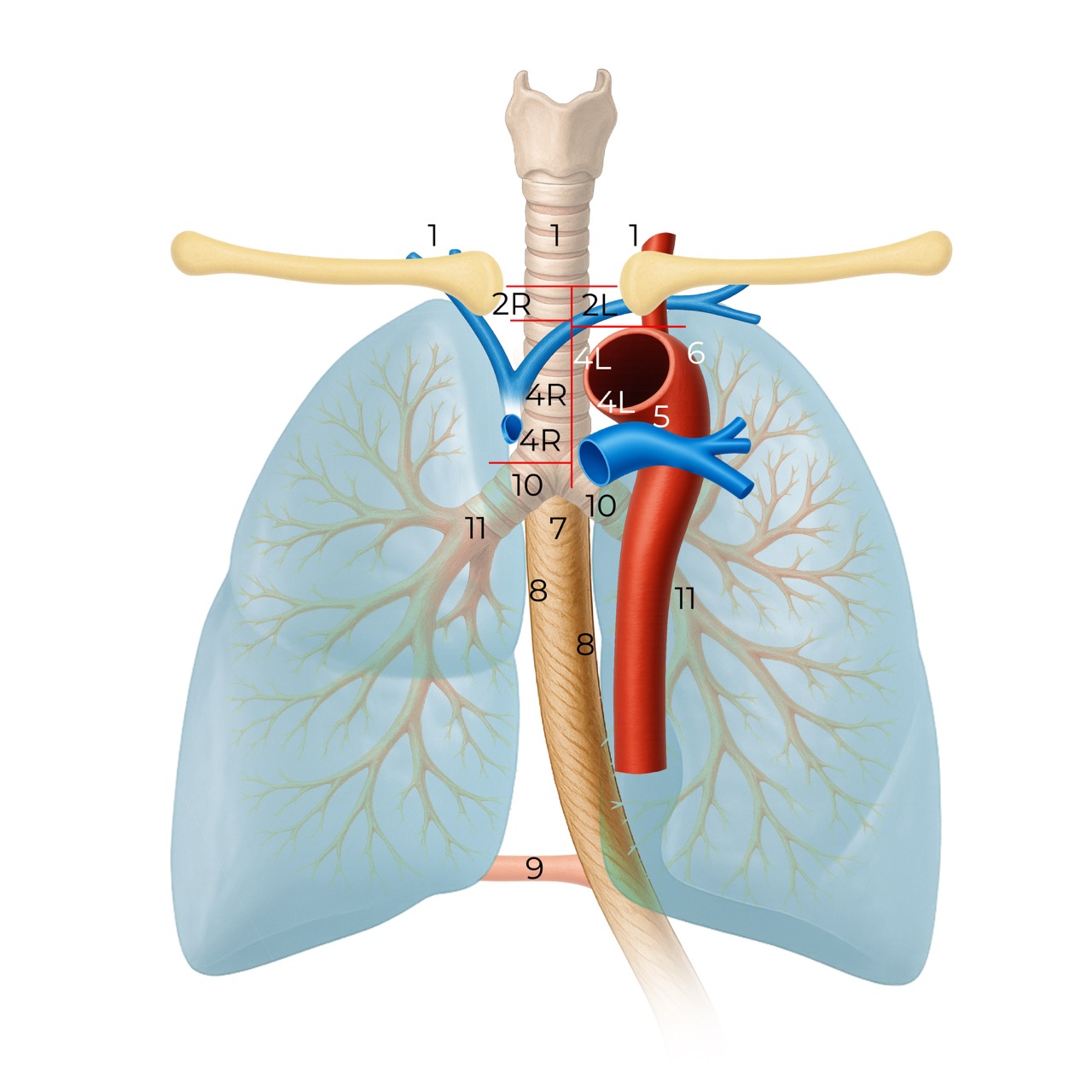
The IASLC lymph node classification is used:
- Low cervical, supraclavicular and sternal notch nodes
- Upper Paratracheal.
- Pre-vascular 3A: nodes not adjacent to the trachea like the nodes in station 2, but anterior to the vessels. Pre-vertebral 3P: nodes not adjacent to the trachea, but behind the esophagus, which is prevertebral (3P).
- Lower paratracheal nodes.
- Subaortic (A-P window) nodes
- Para-aortic (ascending aorta or phrenic) nodes.
- Subcarinal.
- Paraesophageal.
- Pulmonary Ligament: nodes lying within the pulmonary ligaments.
- Hilar nodes: Nodes located outside the mediastinum.
CT is unreliable in staging lymph nodes in patients with NSCLC regardless of the threshold size that is chosen. PET-CT is much more reliable in determining the N-status, although false-positives do occur in patients with for example sarcoid, TB and other infections. PET-CT has a high negative predictive value.
- Level 1: There is an important separation to be made between level 1 (N3) and level 2 and 3 nodes (N2). The lower border of level 1 is the clavicles bilaterally and, in the midline, the upper border of the manubrium.
- Level 2R: The upper border is the apex of lung and in the midline the upper border of the manubrium. The lower border is intersection of the caudal margin of the innominate vein with the trachea. The medial border is along the left lateral border of the trachea.
- Level 2L: From the apex of the lung and the upper border of the manubrium to the superior border of the aortic arch.
- Level 4R: Includes right paratracheal and pretracheal nodes extending to the left lateral border of trachea. From the intersection of caudal margin of innominate vein with the trachea to the lower border of the azygos vein.
- Level 4L: Nodes to the left of the left lateral border of the trachea, but medial to the ligamentum arteriosum. From the upper margin of the aortic arch to the upper rim of the left main pulmonary artery.
- Level 5: Subaortic nodes lateral to ligamentum arteriosum. These nodes are not located between the aorta and the pulmonary trunk, but lateral to these vessels.
- Level 10R: Hilar nodes up to the inferior border of the azygos vein, including those in a precarinal position.
- Level 10L: Hilar nodes extend all the way up to the upper border of the left pulmonary artery.
Practical notes: CT alone is limited for nodal staging; PET-CT improves negative predictive value but can give false positives with inflammatory disease (e.g., sarcoidosis, TB). Pathologic confirmation (EBUS, mediastinoscopy, biopsy) is often required when results would alter management.
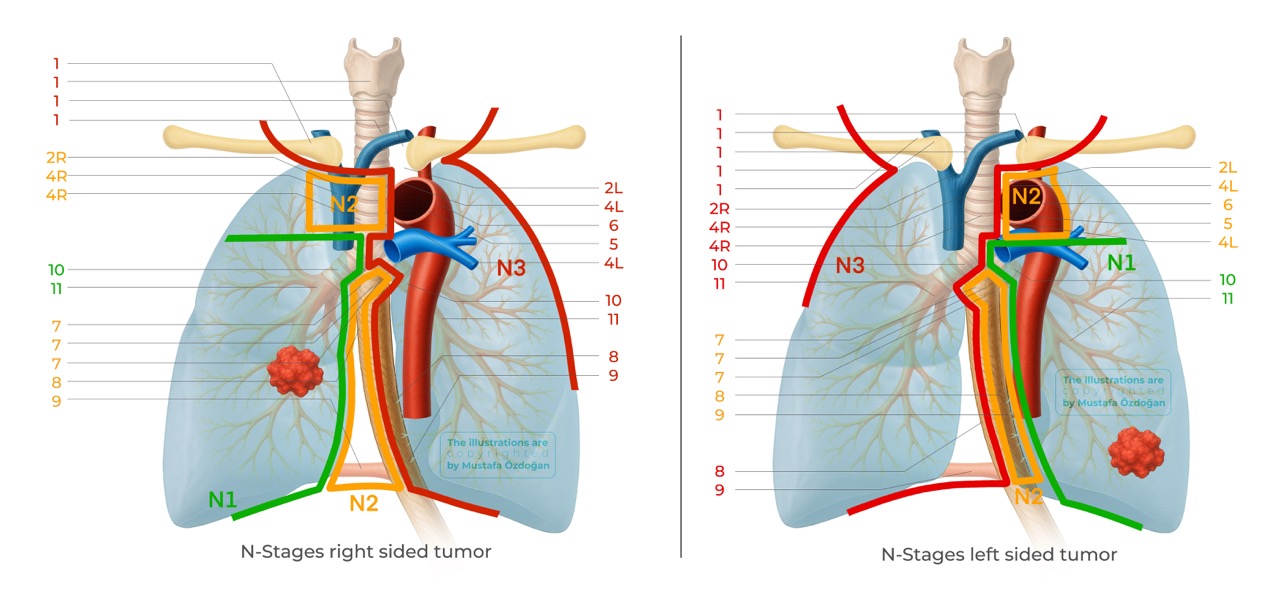
For a tumor in the right lung the N-stages are:
- N1 - Ipsilateral peribronchial and/or hilar lymph nodes 10R-14R
- N2 - Ipsilateral mediastinal and/or midline lymph nodes 2R, 3a/p, 4R, 7, 8R, 9R
- N3 - Contralateral mediastinal and/or hilar, as well as any supraclavicular lymph nodes 1, 2L, 3aL, 4L, 5, 6, 8L, 9L, 10L-14L
For a tumor in the left lung the N-stages are:
- N1 - Ipsilateral peribronchial and/or hilar lymph nodes 10L-14L
- N2 - Ipsilateral mediastinal and/or midline lymph nodes 2L, 3a/p, 4L, 7, 8L, 9L
- N3 - Contralateral mediastinal and/or hilar, as well as any supraclavicular lymph nodes 1, 2R, 3aR, 3pR, 4R, 8R, 9R, 10R-14R
M-Staging (Distant Metastases)
M staging depends on presence, site and multiplicity of distant disease:
- M0: no distant metastasis
- M1a: intrathoracic dissemination — malignant pleural or pericardial effusion, pleural/pericardial nodules, or separate pulmonary nodules in the contralateral lung

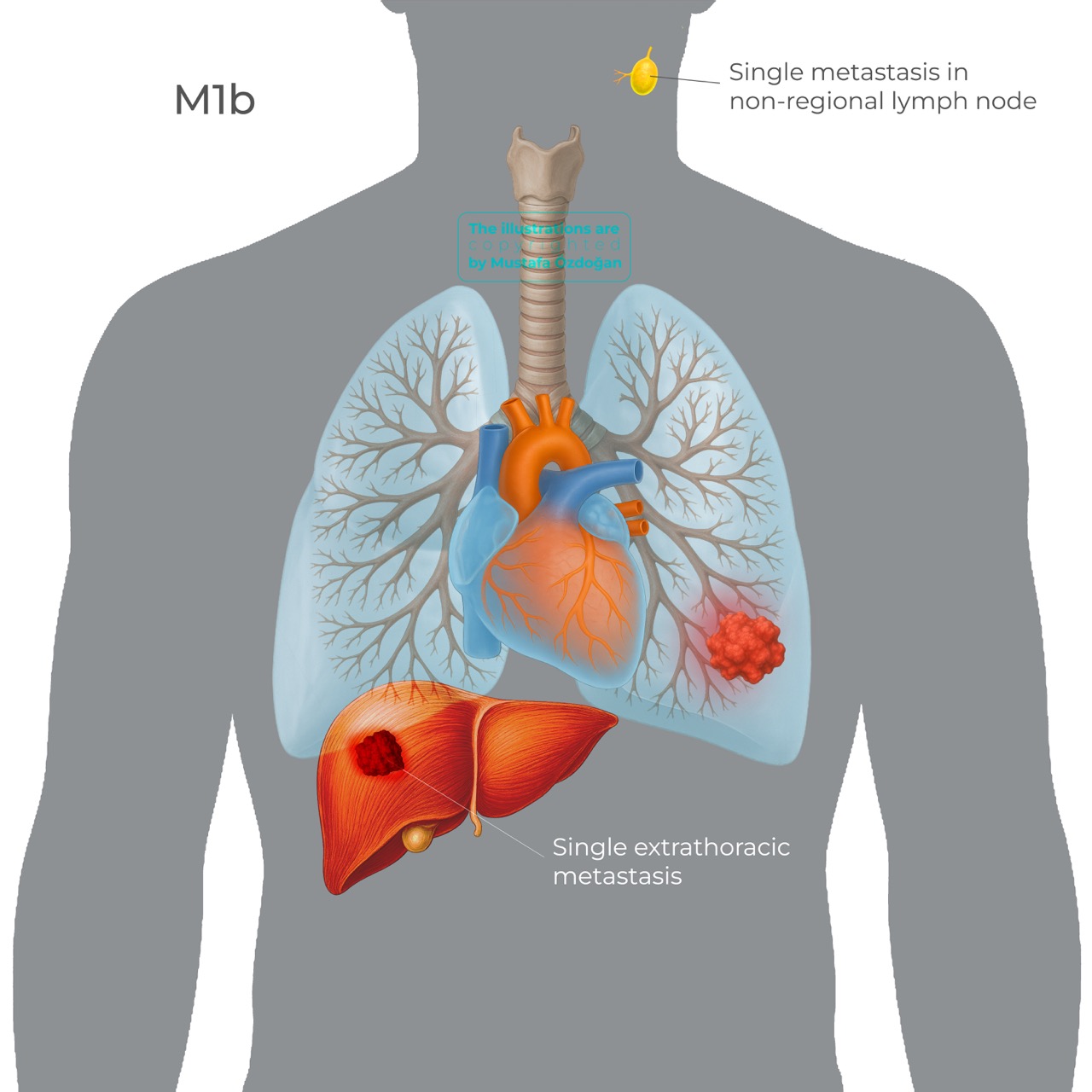
- M1b: single extrathoracic metastasis in a single organ system (e.g., a solitary liver metastasis)
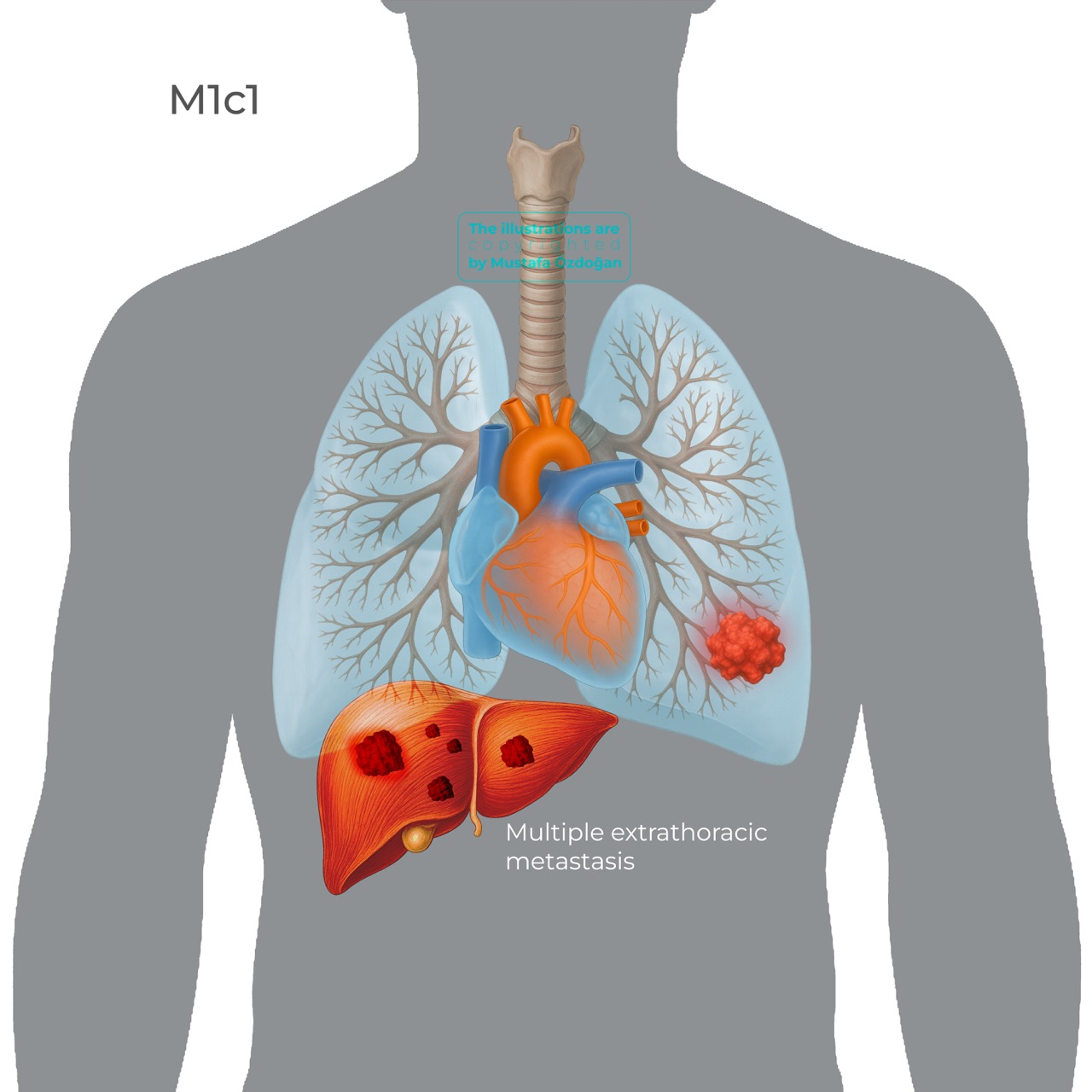
- M1c1: multiple extrathoracic metastases confined to a single organ system (e.g., multiple bone lesions only)
- M1c2: multiple extrathoracic metastases involving more than one organ system
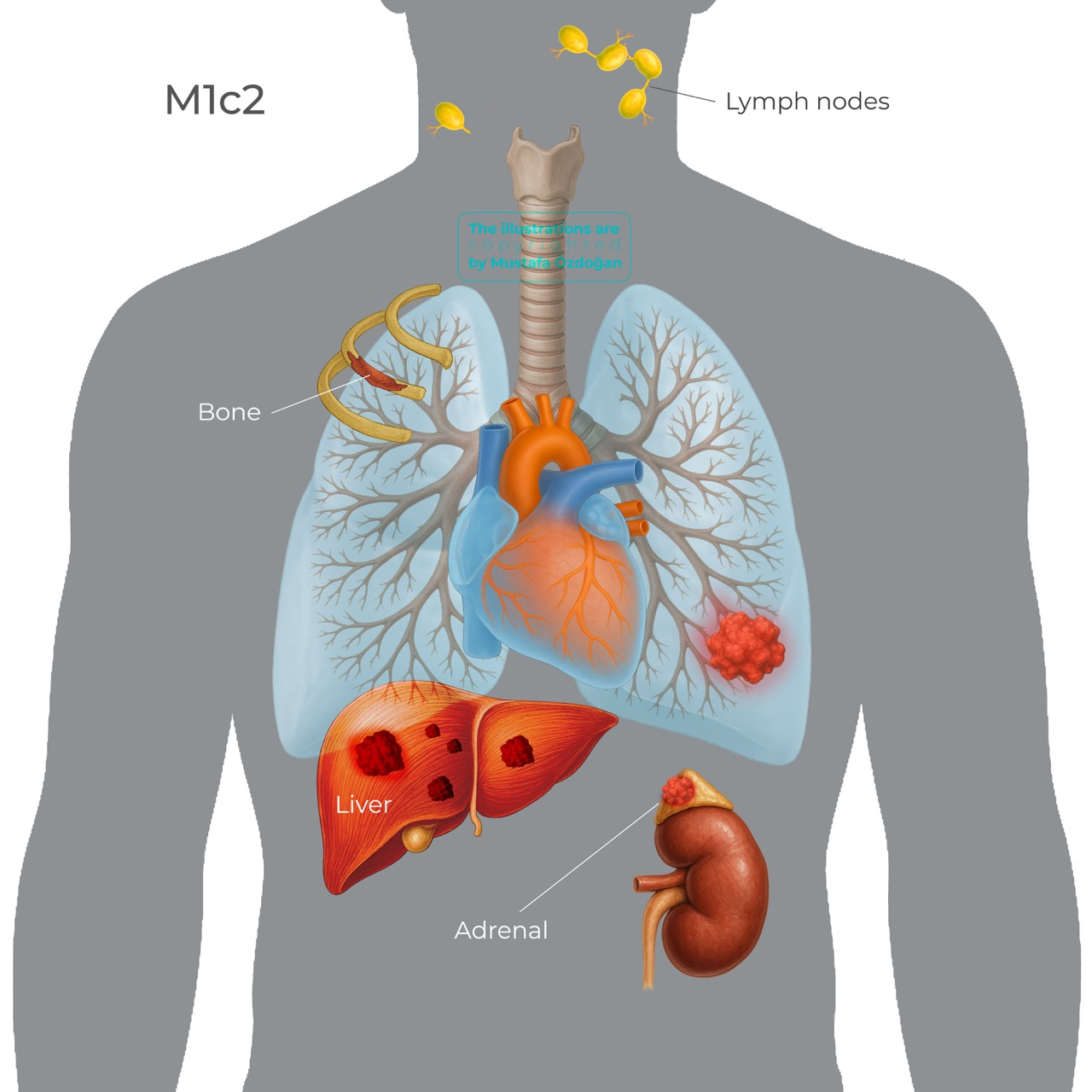
Common metastatic sites include adrenal glands, brain, bone, liver and non-regional lymph nodes.
Stage Grouping (IA → IVB)
Below are the stage group definitions aligned with TNM-9. I preserved clinical meaning while using consistent notation for size ranges and corrected the previously noted phrasing inconsistencies (N0 vs N1 statements, M0 spelling, etc.).
Stage I — IA and IB
Stage IA (cT1 N0 M0) — tumour ≤ 3 cm, peripheral or lobar bronchus, no regional nodes (N0), no distant metastasis (M0).
- IA1 (T1a N0 M0): tumour ≤ 1 cm.
- IA1 (T1mi N0 M0): minimally invasive adenocarcinoma.
- IA2 (T1b N0 M0): > 1 cm and ≤ 2 cm.
- IA3 (T1c N0 M0): > 2 cm and ≤ 3 cm.
Stage IB (T2a N0 M0) — tumour > 3 cm and ≤ 4 cm, or tumour with visceral pleural invasion, involvement of main bronchus (distal to carina), or atelectasis/obstructive pneumonitis extending to the hilum; N0, M0.
Stage II — IIA and IIB
Stage IIA may include:
- T1a–c N1 M0 — tumour ≤ 3 cm with ipsilateral intrapulmonary/peribronchial/hilar nodal metastasis (N1), M0.
- T2b N0 M0 — tumour > 4 cm and ≤ 5 cm (± T2a features), N0, M0.
Stage IIB may include:
- T2a-b N1 M0 — T2a features with N1, M0.
- T3 N0 M0 — T3 tumour (>5–≤7 cm or T3 anatomic invasions/ipsilateral same-lobe nodules), N0, M0.
Stage III — IIIA, IIIB, IIIC
Stage IIIA combinations include (examples):
- T1a–c N2b M0 — small primary with multiple ipsilateral mediastinal/subcarinal stations (N2b), M0.
- T2a/b N2a M0 — T2 tumour with single ipsilateral mediastinal/subcarinal station (N2a), M0.
- T3 N1 M0 — T3 primary with ipsilateral hilar/peribronchial nodes (N1), M0.
- T3N2aM0 — Metastasis to a single ipsilateral mediastinal or subcarinal lymph node station.
- T4 N0/ N1 M0 — T4 primary with N0 or N1, M0.
Stage IIIB combinations include (examples):
- T2a/b N2b M0 — T2 tumour with multiple ipsilateral mediastinal stations (N2b), M0.
- T3/T4 N2b M0 — T3 or T4 with N2b, M0.
- T4N2aM0 — T4 primary with metastasis to a single ipsilateral mediastinal/subcarinal lymph-node station (N2a); no distant metastasis (M0).
Stage IIIC:
T3 N3 M0 or T4 N3 M0 — any of these indicate IIIC (contralateral mediastinal/hilar or supraclavicular nodal involvement with advanced primary).
(Note: precise inclusion of every combined permutation follows the TNM groupings in the IASLC tables; the above lists the representative and commonly encountered combinations.)
Stage IV — IVA and IVB
Stage IVA (M1a or M1b; any T; any N) — intrathoracic spread (M1a: malignant pleural/pericardial effusion or contralateral pulmonary nodules) or single extrathoracic metastasis (M1b). Any T and any N combinations with M1a or M1b are classed IVA.
Representative examples (all require M1a or M1b):
- T1–T4 N0–N3 M1a — intrathoracic metastatic disease (pleural/pericardial disease or contralateral nodules).
- T1–T4 N0–N3 M1b — solitary extrathoracic metastasis (single organ site).
Stage IVB (M1c; any T; any N) — multiple extrathoracic metastases.
- M1c1: multiple metastases confined to a single organ system (e.g., multiple bone lesions).
- M1c2: metastases involving multiple organ systems (e.g., liver + brain). All combinations of T and N with M1c are IVB.
Prognostic Impact of TNM-9
Stage groups correlate strongly with survival estimates: for example, stage IA (cT1N0M0) is associated with approximately 82% 5-year survival, whereas stage IVB (M1c) has much poorer prognosis with roughly 7% 5-year survival. The TNM-9 refinements principally reassign certain T–N combinations across IIA–IIIB, which affects prognostic grouping and treatment decision frameworks.
Conclusion
The 9ᵗʰ Edition of the TNM classification for lung cancer represents an incremental yet meaningful refinement of an already robust system. By incorporating subtle but clinically relevant distinctions (particularly in the N2 and M1 subdivisions) it enhances staging precision and prognostic stratification. These refinements allow for more individualized treatment planning and more accurate comparison of outcomes across studies and institutions. As multidisciplinary approaches and molecular profiling continue to evolve, precise anatomic staging remains the cornerstone upon which therapeutic decisions, clinical trials, and long-term patient outcomes are built.
1. Staging Manual in Thoracic Oncology – 3rd edition
ISBN 9781947768024
2. The Proposed Ninth Edition TNM Classification of Lung Cancer.
Detterbeck et al.
Chest (2024) Oct;166(4):882-895. DOI: 10.1016/j.chest.2024.05.026




