Life-Saving Role of PSMA PET/CT in Treating Biochemical Recurrence of Prostate Cancer
🎯 The Right Treatment for the Right Patient in Prostate Cancer
Prostate cancer is one of the most common cancers in men, and the high rates of biochemical recurrence (rising PSA values after surgery) pose a significant challenge in clinical management. Approximately 30–40% of patients who undergo radical prostatectomy experience a PSA rise, which is an early indicator of cancer recurrence at the microscopic level.
At this stage, the most effective treatment option is salvage radiotherapy (sRT). However, a critical question arises: How can we predict which patients will truly benefit from this therapy? If the disease has spread microscopically beyond the prostate bed, radiotherapy often leads to unnecessary side effects without providing real benefit.
Conventional imaging methods (CT, MRI, bone scintigraphy) are inadequate in detecting recurrence at low PSA levels. Therefore, most patients undergo sRT without prior imaging. However, this often results in ineffective treatments and unnecessary toxicity for some patients.
Graphical Summary
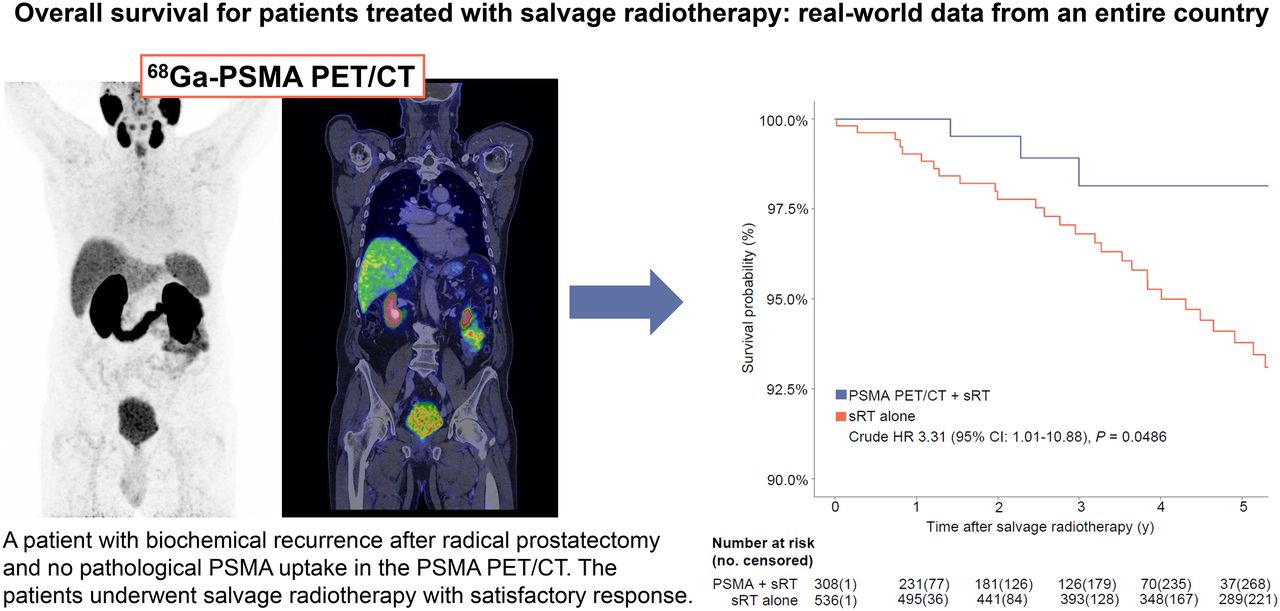
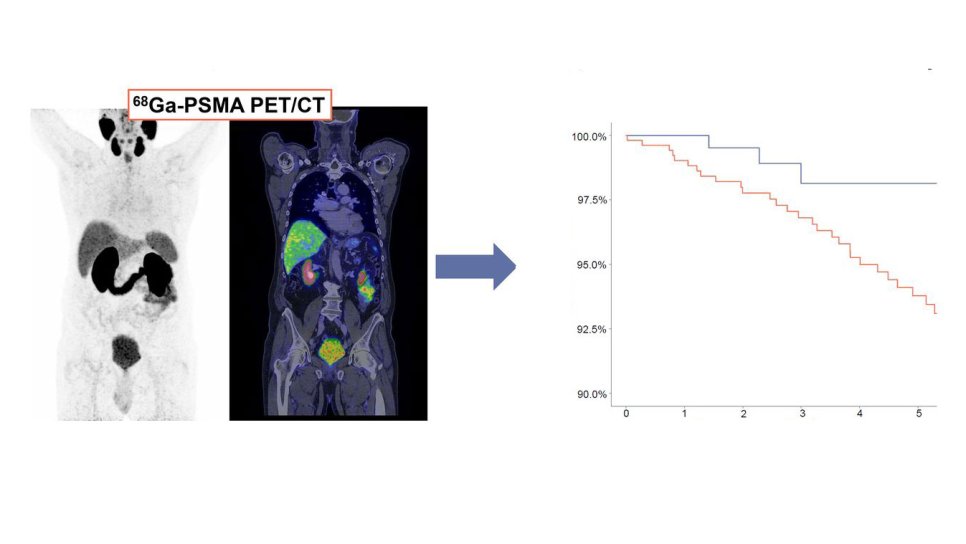
In patients with biochemical recurrence after radical prostatectomy, evaluation with ⁶⁸Ga-PSMA PET/CT enhances the effectiveness of salvage radiotherapy. Patients guided by PSMA PET/CT had significantly higher 5-year overall survival compared to those who received radiotherapy alone (HR: 3.31, p=0.0486). These findings demonstrate that PSMA PET/CT is a critical tool that improves survival by guiding treatment planning.
🔬 The Solution: PSMA PET/CT
One of the most important innovations of recent years, PSMA PET/CT can detect recurrence with high sensitivity even at very low PSA levels. With this tool, physicians can design treatment plans in a more informed and personalized way.
A nationwide study conducted in Denmark and published in Journal of Nuclear Medicine in August 2025 revealed that PSMA PET/CT is not only a diagnostic tool but also a method that creates a survival benefit for patients.
✅ With This Imaging Method:
- The right patients are selected,
- Unnecessary radiotherapy is avoided,
- Treatment becomes more personalized,
- And most importantly: Patients live longer.
💡 These findings strongly indicate that PSMA PET/CT is no longer just a diagnostic tool, but also a game-changing guide in treatment planning.
📊 How Was the Study Conducted?
Design and period: Nationwide, real-world, retrospective cohort conducted between 2015–2023. Data were obtained from Denmark’s national health registries.
👥 Who Was Included?
- Men who had undergone prior radical prostatectomy,
- Biochemical recurrence (BCR): PSA ≥0.2 ng/mL confirmed by at least two measurements,
- Inclusion threshold: PSA 0.2–1.0 ng/mL before salvage RT (sRT),
- Patients receiving radiotherapy for oligometastatic disease were excluded.
🔎 Compared Groups
- Patients who underwent PSMA PET/CT before sRT,
- Patients who did not undergo PSMA PET/CT before sRT.
Note: PSMA PET/CT had to be performed within 6 months of BCR diagnosis and no later than 6 months before sRT initiation.
PSMA tracers used: ⁶⁸Ga-PSMA-11 (since 2015) and ¹⁸F-PSMA-1007 (introduced in some centers since 2020).
Treatment standard: All patients received salvage radiotherapy (sRT) (approximately 30–40 fractions). According to the 2015 guideline update, all patients also received 2 years of ADT (androgen deprivation therapy).
💡 Clinical meaning: Systemic therapy use was similar between groups; the key differentiating factor was more accurate patient and field selection with PSMA.
📌 Sample Size
- Total: 844 patients
- With PSMA PET/CT: 36.5% (n=308)
- Without PSMA PET/CT: 63.5% (n=536)
Baseline characteristics: Groups were similar in age, comorbidities, and pre-surgical parameters. However:
- LN(+) rate was slightly higher in the PSMA group (12.3% vs 9.9%),
- Positive surgical margin rate was lower (50.7% vs 57.5%).
💡 Clinical meaning: Even though the PSMA group had more adverse prognostic factors, outcomes were still better → the key driver was accurate selection with PSMA.
📈 Follow-up and Outcomes
- Primary endpoint: Overall survival (OS) — follow-up started 30 days after completion of sRT.
- Secondary endpoint: Biochemical recurrence-free survival (BRFS) — defined as PSA ≥0.2 ng/mL after sRT.
- Follow-up duration: Median 30 months in the PSMA group vs 68.4 months in the non-PSMA group (due to later adoption of PSMA imaging).
💡 Clinical meaning: Despite the shorter follow-up in the PSMA group, the survival benefit persisted, supporting the robustness of the findings.
📈 Key Findings
✅ Overall Survival (OS)
- Year 1: 100% (PSMA) vs 99% (non-PSMA)
- Year 2: 99.5% vs 97.8%
- Year 5: 98.1% vs 93.8% → Absolute difference: +4.3 points (in favor of PSMA)
Crude hazard ratio (HR): 3.31; p=0.0486
👉 Patients without PSMA had about a 3.3-fold higher risk of death.
Clinical translation:
• The 5-year absolute OS gain of 4.3% is meaningful and clinically valuable.
• Roughly 1 additional life saved for every 23 patients treated (approximate, hypothesis-generating).
✅ Biochemical Recurrence-Free Survival (BRFS)
- 3-year BRFS: 74.9% (PSMA) vs 69.4% (non-PSMA) → Absolute difference: +5.5 points
HR (for recurrence risk): 1.53; p=0.0187
👉 Patients without PSMA had a 53% higher risk of PSA relapse.
- Relative risk reduction:
- At year 1 ≈ 42%
- At year 3 ≈ 18%
💡 Clinical meaning: PSMA-based patient selection provides strong protection particularly in the early years. While the advantage becomes more modest later, it remains durable.
🧠 Why Does PSMA Provide an Advantage?
- 🎯 Accurate targeting: PSMA PET/CT detects hidden tumor foci outside the prostate bed with high accuracy. This allows radiation fields and doses to be planned in the most precise way.
- 🚫 Avoiding unnecessary treatment: Patients unlikely to benefit are spared unnecessary radiotherapy. This prevents both serious side effects (urinary, bowel) and unnecessary costs.
- ⚡ Early and sensitive intervention: Even when PSA is as low as 0.2–1.0 ng/mL, recurrence sites can be detected with high sensitivity, enabling effective treatment at an earlier stage.
🔎 What Do the Findings Mean?
- 📈 Direct contribution to survival: PSMA PET/CT not only shows recurrence, but also guides the right patient to the right treatment at the right time, improving overall survival.
- 👤 Personalized treatment: Identifies which patients will benefit from radiotherapy and prevents unnecessary treatments.
- 🔬 Higher success with early detection: Performing PSMA PET/CT when PSA is still low helps capture recurrence early and increases treatment success.
🩺 Clinical Message
This study provides strong evidence that PSMA PET/CT should become the “new standard” in planning salvage radiotherapy after biochemical recurrence.
📊 A 5-year absolute overall survival difference of 4.3% (98.1% with PSMA vs 93.8% without) represents a critical, life-impacting gain for patients.
Mogensen AW, Torp-Pedersen C, Nørgaard M, Petersen LJ, Moe M, Zacho HD. The Use of PSMA PET/CT Improves Overall Survival in Men with Biochemically Recurrent Prostate Cancer Treated with Salvage Radiotherapy: Real-World Data from an Entire Country. J Nucl Med. 2025;66(8):1217-1222. DOI: 10.2967/jnumed.125.269996