Nivolumab and Ipilimumab in Advanced Gynecologic Clear Cell Carcinomas: MoST-CIRCUIT Trial
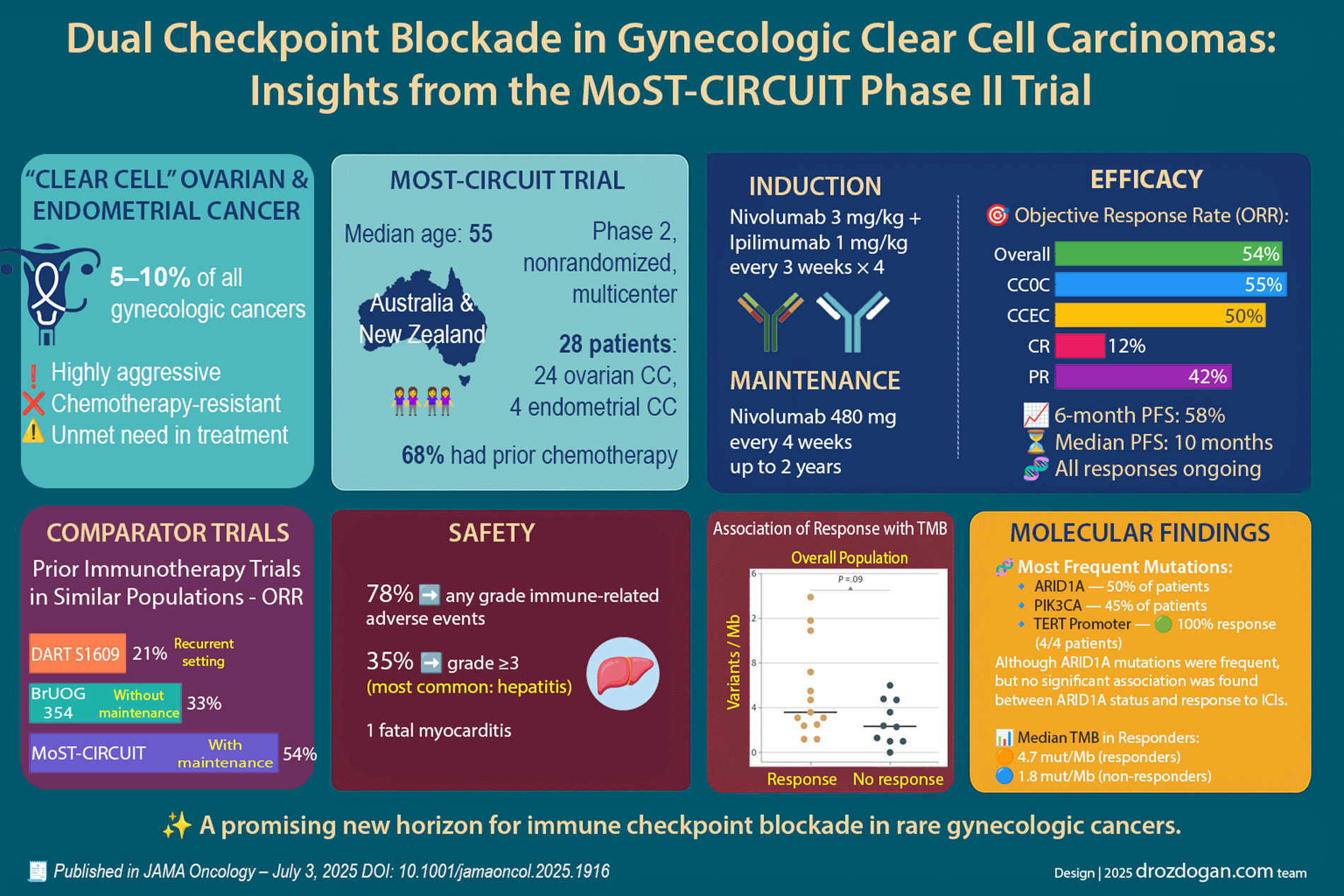
Clear cell carcinomas (CCC) of the ovary and endometrium are both rare and chemoresistant. These tumors respond poorly to conventional cytotoxic therapy and are associated with an unfavorable prognosis even from early stages. To date, durable, highly active systemic options have been lacking.
Against this backdrop, early translational data suggested that immune-checkpoint inhibitors (ICIs) might be particularly effective in this histologic subtype. The phase II MoST-CIRCUIT trial, conducted across multiple Australian centers, therefore tested a dual ICI regimen—nivolumab plus ipilimumab—with maintenance nivolumab. The results are striking.
Published 3 July 2025 in JAMA Oncology (doi: 10.1001/jamaoncol.2025.1916)
Trial Design & Patient Profile
| Design | Phase II, open-label, multicenter, non-randomized |
|---|---|
| Cohort | 28 patients (24 ovarian CCC, 4 endometrial CCC) |
| Median age | 55 years (range 34–77) |
| Prior chemotherapy | 68% (19 patients) |
| Treatment schema | Induction: nivolumab 3 mg/kg + ipilimumab 1 mg/kg q3w × 4 Maintenance: nivolumab 480 mg q4w for up to 2 years |
Efficacy End Points
| Objective response rate (ORR) | 54% (14/26 evaluable) |
|---|---|
| • Complete response (CR) | 12% (3 patients) |
| • Partial response (PR) | 42% (11 patients) |
| ORR—ovarian CCC | 55% |
| ORR—endometrial CCC | 50% |
| 6-month progression-free survival | 58% |
| Median PFS | 10 months |
| Median overall survival | Not yet reached |
| Response durability | All responses ongoing at data cut-off (9–33 months) |
How Does This Compare?
| Trial | ORR | Key distinguishing feature |
|---|---|---|
| MoST-CIRCUIT | 54% | Dual ICI plus maintenance nivolumab |
| BrUOG 354 | 33% | Dual ICI without maintenance |
| DART S1609 | 21% | Single-agent ICI, heavily pre-treated cohort |
The markedly higher response rate in MoST-CIRCUIT likely reflects earlier-line use and inclusion of a maintenance phase.
Safety Profile
| Metric | Incidence |
|---|---|
| Any immune-related adverse event | 78% (22 patients) |
| Grade ≥ 3 immune AEs | 35% (10 patients) — most commonly hepatitis |
| Immune-mediated fatality | 1 myocarditis-related death |
The investigators emphasize the need for vigilant monitoring and prompt ICI-toxicity management when expanding use to new tumor types.
Molecular Insights
- Median tumor mutational burden (TMB): 3.1 mut/Mb (overall low)
- Responders: 4.7 mut/Mb
- Non-responders: 1.8 mut/Mb
- Most frequent pathogenic alterations:
- ARID1A (50%)
- PIK3CA (45%)
- SPOP, ZNF217 (27–23%)
- TERT promoter mutation: detected in 4 patients — 100% response rate. A promising biomarker warranting validation.
Notably, ARID1A status did not stratify response in this cohort, despite prior reports of enhanced ICI sensitivity.
Take-Home Message & Future Directions
This phase II study demonstrates that nivolumab + ipilimumab, followed by nivolumab maintenance, yields deep and durable responses in advanced gynecologic CCC—a disease with otherwise limited treatment options. Although the study is non-randomized and small, its ORR eclipses historical benchmarks, highlighting the regimen’s potential.
Next steps: confirmatory randomized trials and refined biomarker work to delineate which patients benefit most.
For now, dual checkpoint blockade stands out as an emerging therapeutic avenue for these rare, aggressive tumors—offering a much-needed advance where conventional therapies fall short.
Gao B, Carlino MS, Michael M, et al. Nivolumab and Ipilimumab Combination Treatment in Advanced Ovarian and Endometrial Clear Cell Cancers: A Nonrandomized Clinical Trial. JAMA Oncol. Published online July 03, 2025. doi:10.1001/jamaoncol.2025.1916




