Can Early ctDNA Changes Predict Immunotherapy Response in Colorectal Cancer?
Immune checkpoint inhibitors (immunotherapies) have fundamentally changed the treatment landscape, especially in metastatic colorectal cancer (mCRC) patients whose tumors are found to be dMMR/MSI-H.
dMMR/MSI-H is a biomarker characterized by microsatellite instability (MSI-H) and mismatch repair deficiency (dMMR), resulting from impairments in the DNA mismatch repair (MMR) system.
This condition facilitates the immune system's recognition of the tumor, increasing sensitivity to immunotherapies.
Approximately 5% of metastatic colorectal cancer patients present with a dMMR/MSI-H profile.
Although dMMR/MSI-H tumors respond well to immunotherapies, two critical questions still remain unanswered:
- Which patients experience primary resistance to initial treatment?
- When should treatment be discontinued in responding patients?
The answers to these questions are crucial for preventing unnecessary side effects and the rational use of high-cost treatments.
A new hope: Changes in ctDNA (circulating tumor DNA) levels just 1 month after treatment initiation!
These findings were reported in a study published on July 18, 2025, in JAMA Oncology by Taïeb J. and colleagues.
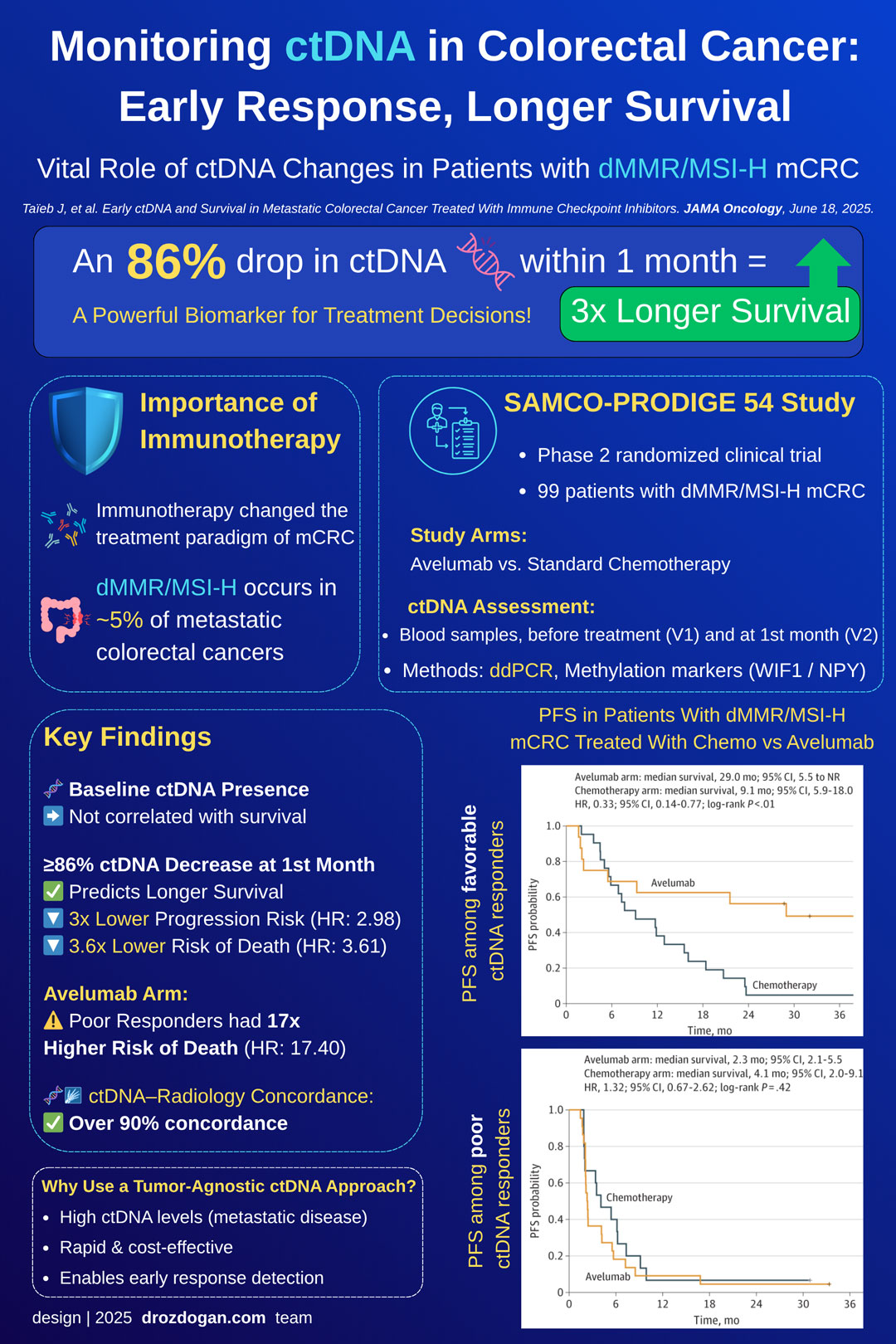
SAMCO-PRODIGE 54 Study
- Phase 2 randomized clinical trial
- Participants: dMMR/MSI-H mCRC patients (99 patients)
- Two arms:
- Avelumab (anti–PD-L1 immunotherapy)
- Standard chemotherapy ± targeted therapy
- Blood samples collected before treatment (V1) and at month 1 (V2)
- ctDNA analysis performed using ddPCR for WIF1 and NPY methylation markers
📊 Key Findings
- Baseline ctDNA presence was not associated with survival.
- However, at month 1, ≥86% ctDNA reduction:
- Progression-free survival (PFS): 3 times lower risk of progression (HR: 2.98; p < .001)
- Overall survival (OS): 3.6 times lower risk of death (HR: 3.61; p < .001)
- In the Avelumab arm: Risk of death was 17 times higher in those with poor ctDNA response (HR: 17.40; p < .001)
- Good ctDNA response was over 90% concordant with radiological response
Clinical Interpretation
- A blood test performed in only 1 month can indicate whether the treatment is working.
- If there's no early ctDNA decrease → consider alternative treatment.
- If there's a strong ctDNA response → treatment duration may be shortened.
- When ctDNA response and radiological assessment (RECIST) are used together, they provide much stronger and more reliable predictions about the disease course.
📉 Summary in Numbers
| Patient Group | PFS (months) | OS (months) | Hazard Ratio (HR) |
|---|---|---|---|
| Good ctDNA Response (≥86% decrease) | 12.0 | Not Reached | Reference |
| Poor ctDNA Response (<86%) | 2.4 | 14.0 | PFS HR: 2.98; OS HR: 3.61 |
| Avelumab + Poor ctDNA Response | 2.3 | 15.0 | OS HR: 17.40 |
⚠️ Limitations
- Relatively small number of participants (99 patients)
- ctDNA was measured only at month 1
- Only Avelumab was tested; other immunotherapies were not included in the study
Conclusion: ctDNA Monitoring Can Be a New Compass
The SAMCO-PRODIGE 54 study revealed that early changes in ctDNA levels in dMMR/MSI-H mCRC patients receiving immunotherapy can predict:
- Treatment response
- Development of drug resistance
- Long-term survival
💡 When ctDNA data are evaluated alongside classical radiological imaging, they can usher in a new era in personalized oncology.
🔍 Technology of the ctDNA Test Used
There are two main approaches to ctDNA analysis:
-
Tumor-informed: Specifically designed based on unique genetic mutations in the patient's tumor tissue. It offers high sensitivity but can be time-consuming and costly.
-
Tumor-agnostic: Does not require any tumor-specific information. It relies on universal genetic or epigenetic markers. It is faster and more suitable for clinical application.
📌 In this study, a tumor-agnostic approach was used. That is, the analysis was performed using ddPCR based on methylation markers (WIF1 and NPY) in ctDNA, without requiring patient-specific mutation analysis from tumor tissue.
🧪 Method Used
- Markers: WIF1 and NPY (methylation patterns)
- Technology: Bisulfite conversion + droplet digital PCR (ddPCR)
- Timing: Pre-treatment (V1) and Month 1 (V2)
This method is considered fast, cost-effective, and easily applicable in clinic, as it does not require mutation analysis from tumor tissue.
💡 Tumor-Agnostic vs. Tumor-Informed Comparison
| Feature | Tumor-Informed | Tumor-Agnostic (In this study) |
|---|---|---|
| Requires tumor tissue? | Yes | No |
| Patient-specific design? | Yes (based on unique mutations) | No (universal methylation markers) |
| Sensitivity | Very High (LOD < 0.01%) | Moderate (LOD ~0.2%) |
| Suitable patient profile | MRD / early-stage patients | Metastatic, high tumor burden |
| Clinical applicability | Difficult, time-consuming | Easy, fast, cost-effective |
✅ Why was the Tumor-Agnostic Method Chosen?
- In metastatic CRC patients, ctDNA levels are generally high → ddPCR is sufficient.
- Fast and inexpensive applicability makes it clinically advantageous.
- Goal: To detect early treatment response.
🎯 ctDNA and MRD in Solid Tumors: New Horizons
While this study generated strong signals, some unanswered questions still remain important:
- What is the best ctDNA testing strategy?
- What are the most appropriate follow-up time intervals?
- Does ctDNA negativity always mean a good prognosis?
- If ctDNA and RECIST are discordant, which should guide decisions?
To answer these questions, larger, prospective, and multi-time-point studies are needed.
However: The data obtained so far provide a strong foundation for the integration of ctDNA into clinical decision support tools.
Taïeb J, et al. Early ctDNA and Survival in Metastatic Colorectal Cancer Treated With Immune Checkpoint Inhibitors. JAMA Oncology, Published online June 18, 2025.